INTRODUCTION
Breast cancer is the most common type of invasive cancer among women and is the second leading cause of cancer-related death. The diagnosis of breast cancer is based on clinical examination combined with imaging and is confirmed by histopathological assessment. Imaging includes bilateral mammography and ultrasonography of the breast and regional lymph nodes (LNs).
Axillary lymph node (ALN) metastasis is an important prognostic factor, and the diagnosis of ALN metastasis is essential for treatment planning, such as start of neoadjuvant chemotherapy or selection of a neoadjuvant chemotherapy agent [1–4].
Although ALN dissection is the standard method of staging in breast cancer, it is associated with postoperative morbidities, such as arm and shoulder pain, lymphedema, paresthesia, nerve injuries, and seroma [5,6]. Sentinel LN biopsy, a less-invasive procedure, is also being used for breast cancer staging, but its clinical application is limited to early-stage breast cancer with no clinical suspicion of ALN metastasis [7,8]. To overcome this limitation, imaging modalities, such as mammography, ultrasonography, and computed tomography (CT), have been used to detect ALN metastasis, but unfortunately, their diagnostic accuracies are limited [9,10].
Fluorine-18 fluorodeoxyglucose (18F-FDG) positron emission tomography-computed tomography (PET-CT) has been widely used for diagnosis, staging, treatment monitoring, and detection of disease recurrence in patients with breast cancer [11–13]. This technique has the advantage of being able to demonstrate abnormal metabolic activities associated with malignancy before the demonstration of abnormal morphological findings by anatomic imaging modalities. In addition, it can show the metabolic activity of the primary tumor and thus predict LN metastasis in various cancers especially non-small cell lung cancer [14].
However, breast cancer is comprised of biologically varying subtypes. Many previous studies have shown a good correlation between 18F-FDG uptake by primary tumor and molecular subtypes of breast cancer [15,16].
The aim of this study was to determine the ability of ALN maximum standardized uptake value (SUVmax) on PET-CT to predict axillary metastasis of breast cancer, and to correlate the results with ultrasonography and clinicopathologic findings.
METHODS
Patients
The records of breast cancer patients who had undergone PET-CT before receiving treatment (surgery and/or chemotherapy) for invasive breast carcinoma at Kyung Hee University Hospital at Gangdong between January 2006 and December 2014 were retrospectively collected and reviewed. The study was approved by the Institutional Review Board of Kyung Hee University Hospital at Gandong (IRB No. KHNMC 2018-10-016) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived. The axillary LNs were preoperatively evaluated by ultrasonography and PET-CT. Lymph nodes were removed by sentinel LN biopsy (SLNB) or axillary LN dissection (ALND) and were histologically diagnosed by experienced pathologists.
Fine needle aspiration
All patients underwent routine preoperative ultrasonography. In cases with suspicious metastatic LNs (above the level of category 4a in the breast imaging-reporting and data system) on preoperative ultrasonography, fine needle aspiration (FNA) of the axilla was done [17].
PET-CT and lymph node/tumor ratio
Whole-body PET-CT was performed within 1 month before treatment. All patients fasted at least 6 hours prior to the PET-CT procedure. After the serum glucose concentration was confirmed as < 150 mg/dL, patients were administered 185 MBq of 18F-FDG intravenously in the arm or leg contralateral to the primary breast tumor and rested quietly for 60 minutes; they then underwent whole-body PET-CT, and the PET-CT images were reconstructed. The FDG uptake in the primary tumor (SUV-T) and lymph node (SUV-LN) was semi-quantitatively analyzed using the SUVmax, which was calculated based on the measured activity, decay-corrected administrated dose, and patient weight. When calculating the SUV-LN, the ALN showing the highest SUV within the whole axillary space was selected. The lymph node/tumor (LN/T) ratio was calculated by dividing the SUV-LN by the SUV-T.
Immunohistochemistry
Estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) expression were assessed by immunohistochemistry (IHC) using a polymer detection system with antibodies against these receptors. ER/PR expression was defined according to the Allred scoring system. The percentage of stained cells (scores, 0–5) and their intensity (scores, 0–3) were determined, and the sum of the intensity and percentage scores was calculated. Allred scores of 0 to 2 were defined as ER/PR negative, whereas scores of 3 to 8 were defined as ER/PR positive [18]. HER2/ErbB2 positivity was defined as an IHC score of 3+ or when the HER2 loci/chromosome 17 centromere ratio was > 2.2. The subtypes of breast cancer were defined as follows [19]: (1) luminal A: ER+ and/or PR+, HER2−, Ki-67 low (< 14%); (2) luminal B: ER+ and/or PR+, HER2−, and Ki-67 high (≥14%); (3) HER2+: ER−, PR−, and HER2+; or (4) triple-negative breast cancer (TNBC): ER−, PR−, and HER2−.
Sentinel lymph node biopsy and axillary lymph node dissection
Each patient underwent either mastectomy or breast-conserving surgery based on the location and extension of the primary tumor. ALND was performed in patients with clinically positive ALNs, while in clinically node negative patients, SLNB was used for axillary evaluation [20]. At our institution, SLNB was performed using a dual-tracer technique, which is a combination of the blue dye method and the gamma probe-guided method. Imaging was performed 1 day preoperatively.
LNs were categorized as suspicious if they exhibited one or more of the following characteristics: cortical thickening or eccentric cortical lobulation with obliteration of echogenic hilum, irregular shape, loss of fatty hilum, or round shape. Patients with pathologically FNA-positive nodes underwent ALND [10,17,21].
Statistical analysis
Student t-test and the chi-square test were used to analyze the sensitivity and specificity. Receiver operating characteristic (ROC) and area under the ROC curve (AUC) analyses were performed. The variables included in the analysis were enumerated. The included variables were mean age at surgery, tumor size, status of LN metastasis, SUV-LN, and SUV-T. SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis of intraclass correlation coefficient. All P-values less than 0.05 were considered statistically significant.
RESULTS
Patient characteristics
The characteristics of the enrolled patients are detailed in Table 1. A total of 348 patients with operable, invasive breast cancer were enrolled, comprising 123 node-positive patients and 225 node-negative patients. The mean age was 52.4 years, and the mean tumor size was 2.33 cm. Patients were staged as follows: stage IA: 144 (41.4%); stage IB: one (0.3%); stage IIA: 103 (29.6%); stage IIB: 49 (14.1%); stage IIIA: 36 (10.3%); stage IIIB: two (0.6%); and stage IIIC: 13 (3.7%). The patients were divided into ER/PR+ low Ki-67: 100 (28.7%); ER/PR+ high Ki-67: 109 (31.3%); HER2+: 67 (19.3%); and TNBC: 72 (20.7%) according to IHC characteristics.
The mean age, surgery, and number of LN metastasis were not significantly different among the subtypes. However, tumor size (2.33 cm) was significantly higher in the HER2+ group (2.67 cm) than in other subtypes (P= 0.041) (Table 2).
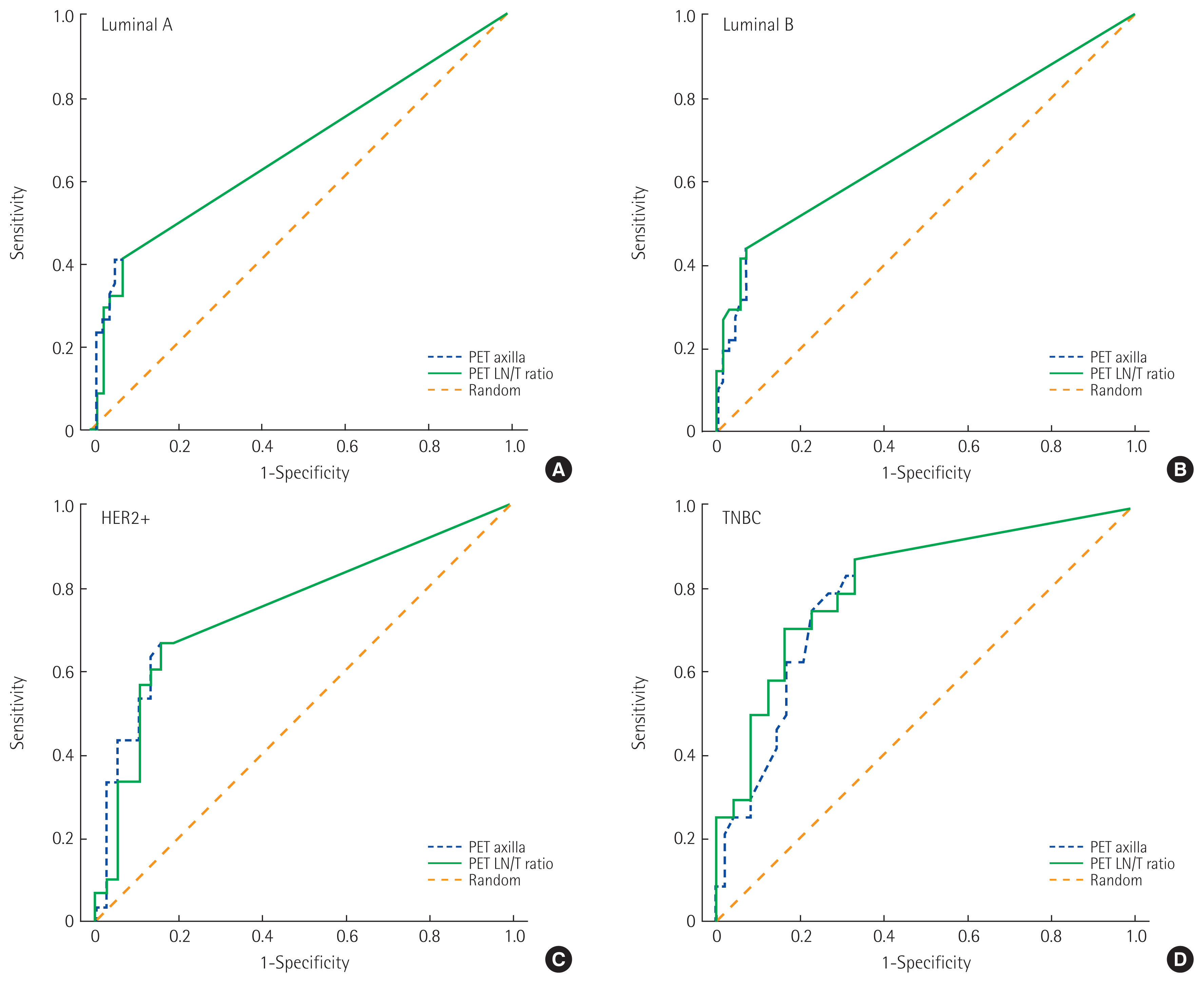
Prediction of lymph node metastasis by PET-CT and ROC curve analysis
Fig. 1 shows the ROC curves used for determining the optimal cutoff values of SUV axilla and the LN/T cutoff values of SUV-LN and LN/T ratio for the detection of ALN metastases. In the luminal A subtype, the AUC for SUV axilla was 0.617 (95% confidence interval [CI], 0.551–0.791) and the LN/T ratio was 0.668 (95% CI, 0.548–0.788). In the luminal B subtype, the AUC for SUV axilla was 0.685 (95% CI, 0.576–0.794) and the LN/T ratio was 0.689 (95% CI, 0.580–0.798). In the HER2+ subtype, the AUC for SUV axilla was 0.761 (95% CI, 0.640–0.882) and the LN/T ratio was 0.750 (95% CI, 0.672–0.873). In the TNBC subtype, the AUC for SUV axilla was 0.797 (95% CI, 0.688–0.907) and the LN/T ratio was 0.817 (95% CI, 0.711–0.923).
The mean SUV-T of the 348 tumors was 4.03±3.33, and the mean SUV-LN was 0.92± 2.00. The corresponding mean SUV-T and SUV-LN are shown in the Table 2. The SUV-T and SUV-LN were significantly higher in the TNBC group than in the other groups (SUV-T: 5.99, P< 0.01; SUV-LN: 1.29, P= 0.014). However, there were no significant differences in the ratio of SUVmax. Metabolic semiquantitative parameters showed a significant correlation with molecular phenotype, with greater SUVs in more biologically aggressive tumors.
Comparison of diagnostic performance
The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of the initial ALN staging were 0.831, 0.273, 0.671, 0.474, and 0.630 on FNA; 0.537, 0.853, 0.667, 0.771, and 0.741 on PET-CT; and 0.881, 0.667, 0.824, 0.757, and 0.804 on FNA+PET-CT, respectively. The sensitivity (0.881), PPV (0.824) and accuracy (0.804) for initial ALN staging were higher for FNA+PET-CT than for other methods.
In PET-CT alone, the subtype with the highest sensitivity (0.870) and NPV (0.917) was TNBC. The AUC of ROC curves for SUV-LN was greatest in TNBC (0.797) (Table 3).
DISCUSSION
The major findings of the present study were that 18F-FDG uptake by breast cancer, expressed as SUVmax, was significantly correlated with many clinicopathological features, and SUV-T and SUV-LN were significantly correlated with the molecular subtypes of breast cancer and were of value in predicting TNBC.
In the past, the treatment of choice for patients with newly diagnosed breast cancer was based on cancer size and presence of LN metastasis [22]. However, tumors in the same stage still comprise a heterogeneous group with different responses to treatment and different overall outcomes. Currently, biological features such as ER, PR, and HER2 status help predict prognoses and identify patients who are more likely to benefit from specific treatment.
Luminal A is the most common subtype of breast cancer, presenting a low expression of genes related to cellular proliferation. Patients with this subtype have a higher survival rate and lower relapse rate than patients with other subtypes because of the good response to hormone treatment [23].
The luminal B subtype has a more aggressive phenotype, higher histological grade, higher proliferative index, and worse prognosis compared to luminal A.
HER2+ breast cancers are characterized by a high expression of the HER2 gene, which promotes tumor growth and progression [24]. They tend to be more aggressive than other subtypes; 75% have a high histological grade, more than 40% have p53 mutations, and they are less responsive to hormone treatment. The HER2+ subtype is clinically associated with a higher rate of recurrence and mortality due to tumor aggressiveness, although the advent of antibody treatment with trastuzumab targeting this receptor has improved survival outcomes in the last decade.
TNBC has a more aggressive biology than other subtypes, is associated with a poor outcome compared to the luminal subtypes [25], and no form of targeted therapy has yet been developed. Basu et al. [26] demonstrated that TNBCs were associated with higher FDG uptake than ER+, PR+, and HER2− tumor, and thus concluded that the enhanced FDG uptake of TNBC is likely related to its aggressive biology.
Various imaging modalities have been used for ALN staging in breast cancer, but the limited diagnostic accuracies have prevented the replacement of surgical ALN staging. Mammography is affected by technique and positioning [27], and the reported sensitivity of mammography and CT for ALN metastasis is low, ranging from 30% to 40% and 50%, respectively [28]. Ultrasonography has been widely used for staging breast cancer, but results are examiner dependent [29], and the reported sensitivity and specificity of ultrasonography for ALN metastasis vary from 49% to 87% and from 56% to 97%, respectively [10]. These imaging modalities primarily depend on LN size or shape for the differentiation of metastatic and nonmetastatic LNs. Therefore, normal or small-size metastatic LNs can be easily missed. Furthermore, the variable morphologic characteristics of LN also reduce accuracy because of the overlapping features of metastatic and nonmetastatic LN [29,30].
SUVmax, a semiquantitative metabolic parameter obtained by 18F-FDG PET-CT, was found to be significantly correlated with the molecular subtype of breast cancer, higher values being evident in more biologically aggressive tumors.
The limited diagnostic performances of PET-CT parameters are attributable to the partial volume effect, relatively low FDG uptake by low-grade malignancies, and FDG uptake by benign entities. Nonetheless, PET-CT provides metabolic information, and hence, combinations of PET-CT and other imaging modalities are expected to improve diagnostic accuracy for ALN metastasis in breast cancer, especially in TNBC.
The present study has several limitations that warrant consideration. First, the study is inherently limited by its retrospective design. Second, partial volume effects were not corrected. Third, CT morphological criteria were not included in the assessment of ALN status. Fourth, we were unable to match LNs evaluated by PET-CT and those that underwent pathologic examination. Instead, we assumed that the ALN assessed with the PET-CT criteria correlated with the overall pathologic diagnosis by surgical specimen.
In conclusion, the characteristics of SUV-T and SUV-LN differed according to the IHC subtype. Compared to other IHC subtypes, the true positivity of axillary metastasis on PET-CT was highest in the triple-negative subtype. These findings could help tailor thee management for individual patients for therapeutic and diagnostic purposes.