Comparison of oncologic outcome of abdominoperineal resection versus sphincter saving resection for low lying rectal cancer
Article information

Abstract
Purpose
The present study compares the peri/postoperative and oncological outcomes of abdominoperineal resections (APR) and sphincter saving resection (SSR) for low lying rectal cancer.
Methods
Between January 2001 and December 2014, 176 patients who underwent SSR (n=67) and APR (n=109) for low rectal cancer, without stage IV, were retrieved from a retrospective database.
Results
With a median follow-up of 66.5 months. The mean total number of harvested lymph nodes was 16.7 (SSR) versus 17.1 (APR) (P=0.801). The advanced T stage was higher in the APR group (82.6%) versus the SSR group (55.2%) (P=0.006). The positive rate of lymph nodes after surgery was significantly higher in the APR group (45.9%) versus SSR group (25.4%) (P<0.05). The 5-year overall survival rates for SSR and APR were 87.3% and 67.6%, respectively (P<0.005). The 5-year disease-free survival rate (DFS) was 83.6% (SSR) versus 65.5% (APR) (P=0.002). The recurrence rate was higher in the APR group (34.9%) versus the SSR group (14.9%) (P=0.004). Local recurrence rate was not different between the two groups. However, distant recurrence rate was significantly higher in the APR group (26.6% vs. 11.9%, P=0.023). In multivariate analysis, node positive (N0 vs. N1–2) was an independent prognostic factor for DFS (P<0.005).
Conclusion
Based on the present data, SSR achieved better 5-year oncological outcome than APR. The positive lymph node ratio in the N stage after surgery was higher in the APR group and this seems to have an effect on the oncological outcomes of the APR group.
INTRODUCTION
The standard surgery for low lying rectal cancer is abdominoperineal resection (APR) which requires a permanent colostomy. However, ultra-low anterior resection (uLAR) with coloanal anastomosis (CAA) and intersphincteric resection (ISR) with CAA have recently been performed for low lying rectal cancer as an anus preserving alternative that avoids the need for permanent colostomy [1,2]. Sphincter saving surgery (SSR) such as uLAR and ISR has recently increased with the better understanding of anal sphincter anatomy, enhanced surgical techniques, and neoadjuvant chemoradiation therapy (CRTx) [3]. Neoadjuvant CRTx contributes to enhancing the success rates of SSR (uLAR and ISR with CAA) by downstaging and downsizing the tumor [4,5]. Although SSR (uLAR and ISR with CAA) has recently been conducted more frequently, this surgery method can increase the potential recurrence risk. Preserving the anal canal and levator ani muscles may potentially damage the distal resection margin (DRM) and circumferential resection margin (CRM) [6–8]. Compared to SSR, APR is considered to enable a longer and more reliable DRM and CRM. It can also resect and obtain more tissue, including the anal canal and the surrounding tissue. Thus, APR is regarded to have a more favorable oncological outcome than that SSR. Nevertheless, in previous studies comparing SSR and APR, several studies reported that the local recurrence and/or 5-year survival rate are worse in APR than SSR for low rectal cancer [9,10]. The aim of the present study is to compare the peri/postoperative and oncological outcomes of APR and SSR for low rectal cancer.
METHODS
Between January 2001 and December 2014, 176 patients that underwent curative surgical resection (uLAR, ISR, and APR) for low rectal adenocarcinoma (≤5 cm from anal verge) were identified from a retrospective database. Stage IV patients in the present study were excluded. Among the study participants, 67 patients underwent SSR (uLAR and ISR with CAA) and 109 patients underwent APR. All data of the clinical and pathological features were reviewed retrospectively. All patients underwent colonoscopy and biopsy, staging scans (computed tomography scan chest, abdomen and pelvis/magnetic resonance imaging pelvis) and occasionally positron emission tomography-computed tomography scans. The neoadjuvant CRTx was performed with long course CRTx (5-fluorouracil based chemotherapy, 50.4 Gy) as the patients were clinically T3 or T4 and/or node positive. Repeat scans were performed after a minimum of 4 weeks of CRTx completion. Surgery was performed 6 to 8 weeks after completion of CRTx. All patients received full bowel preparation and a single shot of prophylactic antibiotics. All patients underwent complete total mesorectal excision. Adjuvant chemotherapy was performed on a 5-fluorouracil and leucovorin-based regimen (six cycles of monthly bolus intravenous 5-fluorouracil [400–425 mg/m2/day], days 1–5; and leucovorin [20 mg/m2/day], days 1–5). The adjuvant chemotherapy was not performed in the cases of old age or patient refusal or side effects. Patients received close follow-up and were recorded on a database till death or May 2018. Disease-free survival (DFS) was defined from the date of surgery to the date of the detection of recurrence or last follow-up or death. Patients in the two groups undergoing SSR (uLAR and ISR with CAA) and APR were compared with respect to demographics and oncological outcomes.
All statistical analyses were performed using SAS version 9.1.3 (SAS Institute Inc., Cary, NC, USA) and SPSS software, version 24.0 (IBM Corp., Armonk, NY, USA). Categorical variables were analyzed using the chi-square or Fisher exact test, and continuous variables were analyzed using the Student t-test and Mann-Whitney U rank test. Cumulative-incidence methods were used to estimate the rate of cancer recurrence. Overall survival (OS) and DFS were analyzed using the Kaplan-Meier method, and comparison was performed using the log-rank test. P-values of less than 0.05 were considered statistically significant.
RESULTS
Patient characteristics
Comparative analysis was conducted regarding the characteristics of the patients of the SSR group (n=67) and APR group (n=109) (Table 1). Mean age, sex ratio, height, weight, body mass index (BMI), and American Society of Anesthesiologists scores, as well as initial carcinoembryonic antigen level, were not significantly different between the two groups. The rate of patients who received neoadjuvant CRTx was significantly higher in the SSR group (52.2%) than in the APR group (14.7%) (P<0.005).
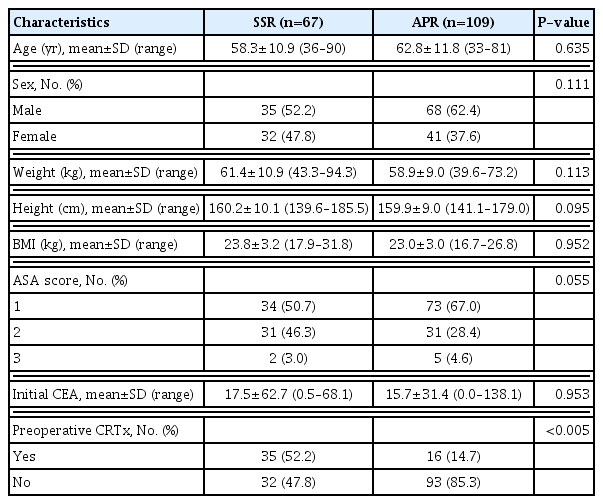
Patient characteristics (n=176)
Pathologic results
The tumor-node-metastasis (TNM) stage, pT stage, pN stage, and pM stage were classified according to the American Joint Committee on Cancer (AJCC, 7th edition) staging system. Regarding the TNM stage distribution, the T stage was significantly different between the two groups (P<0.006) with more advanced stage in the APR group (T3 stage; 52.2% vs. 73.4%). As to the overall stage, the APR group showed a significantly higher proportion of advanced stage compared to the SSR group (IIIb; 13.4% in SSR vs. 34.9% in APR, P<0.003). There was no significant difference between the two groups regarding N stage (P=0.071) (Table 2). However, the rate of N (+) was higher in the APR group (n=50, 45.9%) than in the SSR group (n=17, 25.4%) (P<0.05). The histological grades of differentiation, perineural invasion rate and harvested number of lymph node were not significantly different between the two groups. The lymphovascular invasion rate was significantly higher in the APR group compared to the SSR group (APR 32.1% vs. SSR 16.4%, P=0.021). The proximal resection margin (APR 20.7 cm vs. SSR 14.1 cm, P=0.001) and DRM (APR 3.7 cm vs. SSR 2.1 cm, P=0.008) were longer in the APR group than the SSR group. Mass size and CRM were not significantly different between the two groups (Table 2).
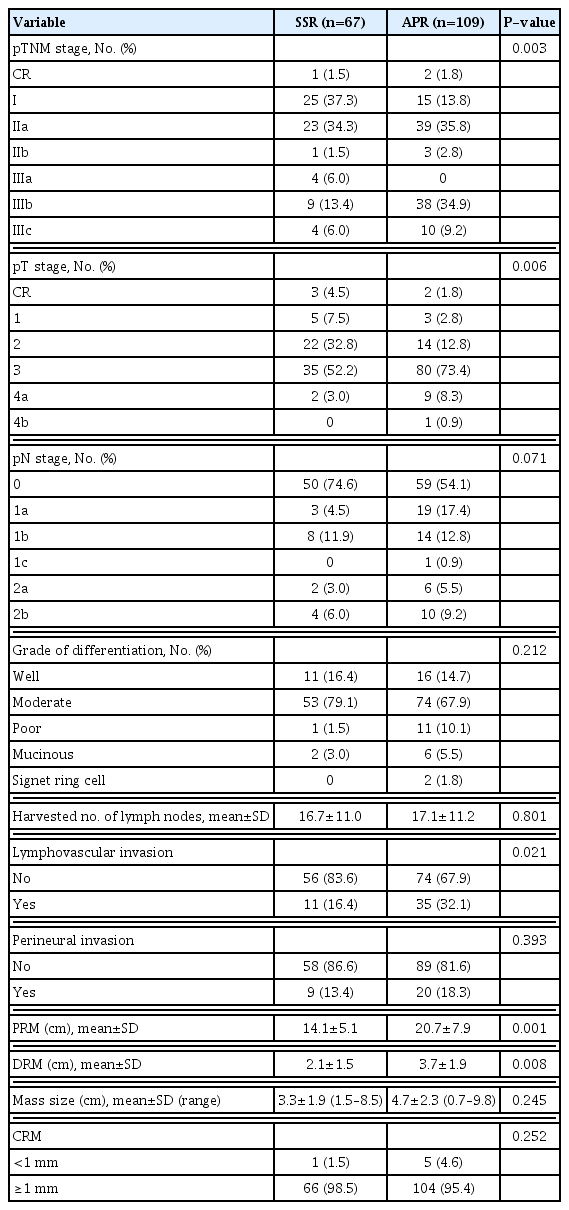
Postoperative pathologic outcomes after surgery for low rectal cancer
Oncological outcomes
The mean follow-up period was 66.5 months. The 5-year OS rate was significantly higher in the SSR group compared to the APR group (87.3% vs. 67.6%, P<0.005). The 5-year DFS rate was also significantly higher in the SSR group than the APR group (83.6% vs. 65.5%, P<0.002) (Fig. 1). In the node negative stage, the 5-year OS rate (SSR 92.3% vs. APR 87.1%, P=0.100) and DFS rate (SSR 88.2% vs. APR 87.3%, P=0.488) were not significantly different between the two groups. In the node positive stage, the 5-year OS rate (SSR 74.2% vs. APR 45.2%, P<0.005) and DFS rate (SSR 70.6% vs. APR 39.6%, P<0.005) were significantly higher in the SSR group (Fig. 2). Regarding the oncological outcomes of neoadjuvant CRTx, patients that received neoadjuvant CRTx compared to those that did not showed significantly better results. The 5-year OS rate was 90.9% in patients that received neoadjuvant CRTx and 68.7% in those that did not receive neoadjuvant CRTx (P=0.001). The 5-year DFS rate was 83.0% in patients that underwent neoadjuvant CRTx treatment and 68.1% in those that did not (P=0.026) (Fig. 3).
Oncologic outcome between sphincter saving surgery (SSR) and abdominoperineal resection (APR) groups. (A) Overall survival rate and (B) disease-free survival rate.

Oncologic outcome between sphincter saving surgery (SSR) and abdominoperineal resection (APR) groups according to N stage. (A, B) Five-year overall survival rate and disease-free survival rate for N (−) stage. (C, D) Five-year overall survival rate and disease-free survival rate for N (+) stage.

Oncologic outcome of ultra-low anterior resection and abdominoperineal resection groups according to chemoradiation therapy (CRTx).
Recurrent patterns of SSR versus APR for low rectal cancer
The total recurrence rate was significantly higher in the APR group compared to the SSR group (34.9% vs. 14.9%, P=0.004). The APR group also showed a significantly higher systemic recurrence rate (26.6% vs. 11.9%, P=0.023). The local recurrence rate was not significantly different between the two groups (9.2% vs. 3.0%, P=0.114). The organs of systemic recurrence were the lung, liver, para-aortic node, spine and inguinal node. The recurrence of the lung was observed in six patients (9.0%) of the SSR group and in 13 patients (11.9%) of the APR group. Liver recurrence was observed in two patients (3.0%) of the SSR group and in seven patients (6.4%) of the APR group. The recurrence of the para-aortic node was observed in three patients (2.8%) of the APR group. Spinal recurrence was observed in one patient (1.5%) of the SSR group and in three patients (2.8%) of the APR group. The recurrence of the inguinal node was observed in two patients (1.8%) of the APR group. The sites of local recurrence included the pelvic side wall, perineum, rectal fossa, and anastomosis site. The recurrence of the pelvic side wall was found in one patient (1.5%) of the SSR group and in two patients (1.8%) of the APR group. The recurrence of the perineum was in three patients (2.8%) of the APR group. The recurrence of the rectal fossa was in five patients (4.6%) of the APR group. The recurrence of anastomosis site was in one patient of the SSR group (1.5%) (Table 3).
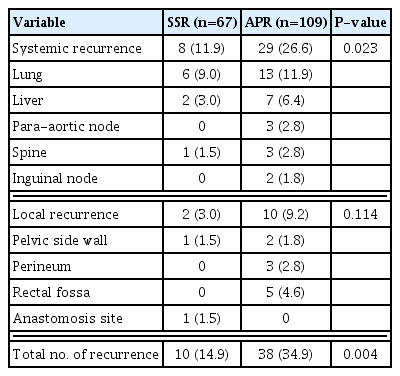
Recurrence pattern of SSR versus APR for low rectal cancer
Positive rate of pathologic lymph nodes associated with neoadjuvant CRTx
The node positive rate after surgery was significantly higher in patients that did not receive neoadjuvant CRTx (n=54, 43.2%) compared to those that did undergo the treatment (n=13, 25.5%) (P=0.020). The node negative rate after surgery was 74.5% (n=38) in patients that received neoadjuvant CRTx, and 56.8% (n=71) in patients that did not receive the treatment. The rate of patients who received neoadjuvant CRTx in the SSR group (n=35, 52.2%) was significantly higher compared to the APR group (n=16, 14.7%) (P<0.005). The node positive rate after surgery was significantly higher in the APR group (n=50, 45.9%) compared to the SSR group (n=17, 25.4%) (P<0.05) (Table 4).

Positive rate of pathologic lymph nodes associated with neoadjuvant CRTx
Univariate and multivariate analyses for prognostic factor
In univariate analysis, BMI, tumor size, advanced T stage, N (+) stage, histologic grade, lymphovascular invasion, perineural invasion, and neoadjuvant CRTx treatment were prognostic factors of DFS after surgery for low lying rectal cancer. In multivariate analysis, BMI and N (+) stage were significant prognostic factors of DFS (Table 5).
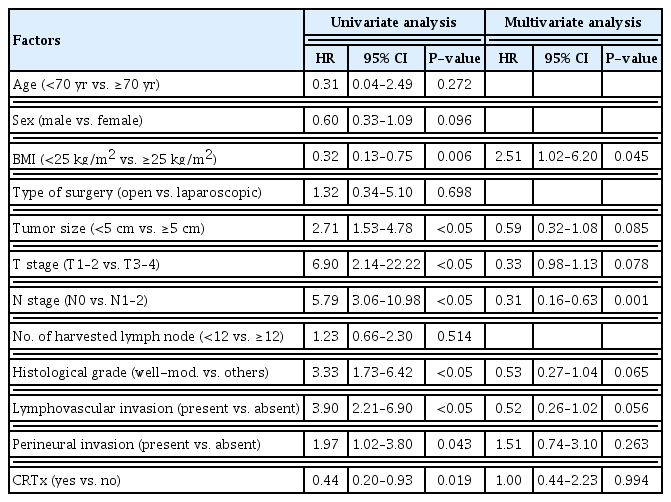
Univariate and multivariate analysis for prognostic factor of disease-free survival after surgery for low lying rectal cancer
DISCUSSION
Decisions regarding the appropriate surgical method for low lying rectal cancer are difficult to make. Oncologic surgery was designed for the purpose of radical resection, but recent oncologic surgery strives to preserve organs as much as possible. Regarding surgical procedures, APR and SSR share similar total mesorectal excision (TME) procedures which include the mesorectum tapering into the plane between the levator-sphincter junctions and intersphincteric plane. However, differences arise during the perineal procedure of APR during which the anal canal and the surrounding tissue may be obtained. Therefore, APR is expected to be more advantageous in terms of oncological outcomes after surgery by obtaining a longer DRM and a more secure CRM.
However, in the present study, the SSR group showed better oncological outcomes than the APR group. DRM was longer in the APR group compared to the SSR group (APR 3.7 cm vs. SSR 2.1 cm, P=0.008). The type of surgery for lower rectal cancer is largely determined by R0 resection and tumor location with adequate DRM (usually 2 cm allowed) [11]. However, this concept of a 2 cm DRM for lower rectal cancer has been challenged by many studies in the setting of neoadjuvant therapy. Study cases of locally advanced rectal cancer after receiving neoadjuvant CRTx reported that 21% of patients had distal margins less than 1 cm without a positive distal margin, and the extent of the DRM was not associated with DFS [12,13]. In the present study, although the APR group showed longer distal margin than the SSR group, this does not seem to have an effect on the oncological outcome.
Some studies have shown that APR is associated with increased local recurrence and decreased cancer-specific survival rate compared to LAR [9,14]. A propensity score matched SEER analysis reported worse oncological outcomes in patients with APR compared to CAA. The 5-year OS rate was 65.6% in APR versus 76.7% in CAA (P<0.001) [15]. The GRECCAR 1 study reported that OS rate and DFS rate were significantly higher for SSR (72.2% and 60.1%) compared APR (54.7% and 38.3%, respectively) [16].
In the present study, 5-year OS rate and DFS rate of APR (OS 67.6%, DFS 65.5%) were significantly worse compared to SSR (OS 87.3%, DFS 83.6%). The local recurrence rate was not significantly different between the APR and SSR groups (APR 9.2% vs. SSR 3.0%, P=0.114). However, the systemic recurrence rate was significantly higher in the APR group (APR 26.6% vs. SSR 11.9%, P=0.023). In another study similar to the present study, there was no difference in local recurrence but systemic recurrence was reported higher for APR than SSR (APR 29.1% vs. SSR 6.1%) [17]. Other studies reported that APR itself was not associated with increased local recurrence or reduced OS [18].
Regarding this study, the lymphovascular invasion rate was also significantly higher in APR than SSR (APR 32.1% vs. SSR 16.4%, P=0.021). The most common site of systemic recurrence was lung metastasis in both groups (APR 11.9%, SSR 9.0%). It is known that lower rectal cancer has dual venous drainage channels with portal and systemic communications through the superior rectal and internal iliac vein, respectively [19]. The lung is the most common site of extra-abdominal metastases in patients with colorectal cancer, and it occurs more often in patients with rectal cancer than colon cancer [20]. With higher lymphovascular invasion rates, higher systemic recurrence rates may be expected.
The CRM positive rate after surgery for rectal cancer was an important factor of recurrence and oncological outcome in a previous meta-analysis study [21]. In the present study, CRM positive rate was not significantly different between the APR and SSR groups (APR 4.6% vs. SSR 1.5%, P=0.252). Although it is more convenient to obtain CRM through APR, it is not difficult to obtain CRM with SSR. Moreover, the neoadjuvant CRTx may further reduce differences regarding the CRM positive rate. It seems that the difference in surgical type (APR or SSR) does not significantly affect CRM in the present study.
In another study of lower rectal cancer patients treated by neoadjuvant CRTx and TME, the 5-year release-free survival rates for the SSR, ISR, and APR groups were reported as 85%, 83%, and 47%, respectively (P=0.001) [22]. This study suggested the relatively poor oncological outcome of the APR group was due to the fact that patients with good response for neoadjuvant CRTx received ISR and those with poor response received APR. Neoadjuvant CRTx is effective in downstaging, increasing resection rate and local control rate, especially for patients with low rectal cancer, and thus increases the OS rate for certain patients [4,23,24]. Neoadjuvant CRTx can downstage tumors, which is illustrated with the decreased thickness of invaded intestinal wall and decreased numbers of metastatic lymph nodes. Lymph node metastasis (or N stage) is a significant prognostic factor for local recurrence, distant metastasis and OS rate [25–27].
In the present study, the rate of patients who received neoadjuvant CRTx in the SSR group was significantly higher compared to the APR group (SSR 52.2% vs. APR 14.7%) (P<0.005). The lower neoadjuvant CRTx rate in the APR group is because sphincter preservation is not necessary in a situation where en-bloc resection is judged to be possible in clinical stage. Due to this reason, surgery is first performed without neoadjuvant CRTx and then adjuvant chemotherapy is performed according to the pathologic stage. The lymph node (or N stage) positive rate after surgery was significantly higher in patients who did not receive neoadjuvant CRTx (n=54, 43.2%) compared to patients who received neoadjuvant CRTx (n=13, 25.5%) (P=0.020). When the patients were divided into groups according to CRTx treatment, the oncological outcome was significantly better in the CRTx treatment group. It is estimated that the oncological outcome of the APR group was worse than that of the SSR group because the lymph node positive (or N stage) rate was higher and the CRTx treatment rate was lower than the SSR group. The present study has several limitations. It is a retrospective, single-center study with small sample size and has significant selection biases.
In conclusion, the 5-year oncological outcome of the SSR group showed better results than the APR group. The higher positive rate of lymph nodes in N stage after surgery and the lower rate of neoadjuvant CRTx seem to have an effect on the oncological outcomes of the APR group.
ACKNOWLEDGMENTS
This work was supported by the Soonchunhyang University Research Fund.
Notes
No potential conflict of interest relevant to this article was reported.