Retroperitoneal sarcomas: Outcomes of repeated resections
Article information

Abstract
Purpose
Retroperitoneal sarcomas (RPS) are rare malignant tumors arising from mesenchymal cells. The objective of this study was to review the treatment experiences and to identify prognostic factors for overall survival (OS) after primary resection and subsequent reoperations for recurrences.
Methods
The medical records of patients who underwent resection for RPS at our institution between June 2002 and December 2016 were retrospectively reviewed. Univariate and multivariable Cox proportional hazards modeling was used to assess the prognostic factors for OS.
Results
A total of 48 patients were enrolled. On multivariable analysis in primary resection group, the FNCLCC (Fédération Nationale des Centres de Lutte Contre le Cancer) grade was a significant prognostic factor for OS (P=0.006). The patients who received chemotherapy after primary resection were significantly associated with poor prognosis (P=0.009). The 5-year OS rate after primary resection (n=48) were 58.1% and the 5-year cumulative reoperation rate after primary resection was 62.5%. After second resection for recurrence after primary resection (n=23), the 5-year OS rate was 64.3%. There was a tendency towards decreased surgery-free survival rate as the number of repeated resections for recurrent RPS increased. In the subset of patients (n=16) who underwent more than 3 repeated resections at our institute, the 5-year OS rate was 75.0%, indicating that repeated resections are not associated with worse outcome.
Conclusion
Only low tumor grade was an independent favorable prognostic factor for OS. Although the prognosis for RPS remains poor, repeated resections for recurrence are not associated with poor prognosis. Aggressive surgical strategies for recurred RPS patients are warranted.
INTRODUCTION
Retroperitoneal sarcomas (RPS) are rare malignant tumors arising from mesenchymal cells of the retroperitoneum such as muscle, fat, and other connective tissue and have a low incidence of 0.5 to 1 cases per 100,000 [1,2]. Complete surgical resection of the tumor and involved adjacent structures or organs is the standard of treatment for patients with localized RPS [3,4]. However complete resection is difficult because the tumors are usually asymptomatic until they reach large dimensions [5]. As such, the tumors are often large at presentation and anatomically close to important structures and organs [6].
The prognosis for patients with RPS is relatively poor, with 5-year overall survival (OS) rates reported in the range of 39% to 70% from series with long-term follow-up [7]. Similarly, in Korea, 5-year OS rates for RPS patients are 30% to 87% [8–11]. Several factors have previously been reported to affect OS including age, histologic type, grade, tumor size, and resection type [2,5,6]. However, there are only a few studies on RPS in Korea since there is no specialized center for RPS. The purpose of this study was to review the treatment experiences of RPS in a large volume center in Korea and to identify prognostic factors for OS after primary resection of tumor and subsequent reoperations for recurrences.
METHODS
We retrospectively reviewed prospectively collected data of patients who underwent operations with curative intent for RPS at Seoul National University Hospital in Korea between June 2002 and December 2016. Retroperitoneal tumors other than sarcomas were excluded. This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1906-014-1036). The informed consent was waived.
The following variables were evaluated: age, sex, initial presenting symptoms, duration of presenting symptoms, histologic type, tumor grade, tumor size, resection type (R0/R1, R2), radiation therapy and chemotherapy after resection, pathologic organ invasion and contiguous organ resection. The resection type was divided into complete gross resection (R0/R1) and incomplete resection (R2). Tumor grade was assessed according to the Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC) system based on differentiation, necrosis, and mitotic rate [12,13]. Recurrence was defined as the presence of a tumor confirmed by imaging study after resection, and patients with recurrence underwent reoperation when feasible. We divided the patients into two groups, the primary resection group and the repeated resection group (defined as patients who underwent additional resections for recurrence after primary resection). OS was calculated from the date of operation to the date of death or last follow-up.
Statistical analysis was conducted using SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA). P-value <0.05 was considered statistically significant. OS rate was estimated using the Kaplan-Meier method. Univariate and multivariate prognostic factor analyses for OS were performed using the log-rank test and Cox proportional hazards model, and the multivariable analysis included factors with a P-value <0.1 in the univariable analysis.
RESULTS
Of the 50 patients with primary RPS, two patients were excluded from this study because of insufficient operation records or pathologic reports. Of the 48 patients who received primary resection at our institution, 23 patients (47.9%) underwent repeated resections for recurrences during the follow-up period (Fig. 1).
Flowchart of patient management (June 2002 to December 2016). SNUH, Seoul National University Hospital.
Prognostic factors after primary resection
The clinicopathologic characteristics of the 48 patients who underwent primary resection at our institution are shown in Table 1. There were 22 males (45.8%) and 26 females (54.2%) with a mean age of 54 years (range, 21–84 years). Thirty-three patients (68.8%) had initial symptoms including diffuse abdominal pain (n=15, 31.3%), palpable mass (n=15, 31.3%), and nonspecific gastrointestinal symptoms (n=3, 6.2%). Eleven patients (22.9%) were asymptomatic, and the tumor was incidentally discovered.
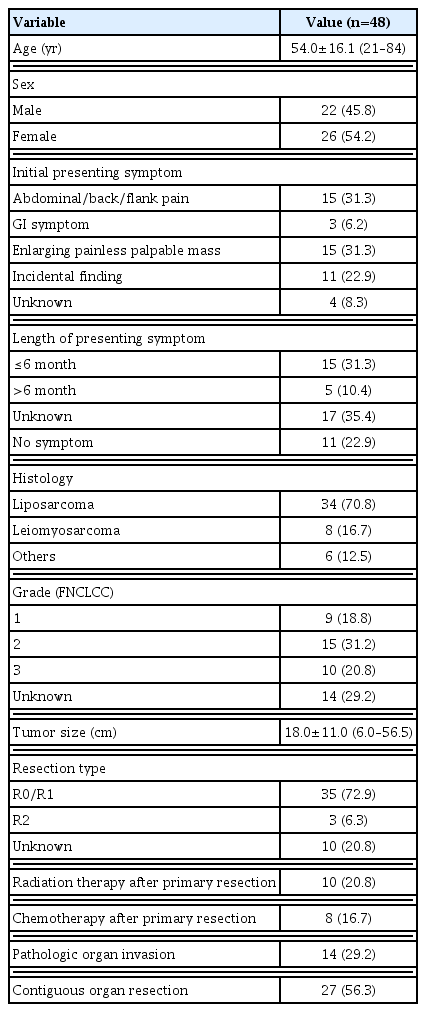
Clinicopathologic characteristics of patients who underwent primary resection for retroperitoneal sarcoma
The mean size of the resected tumors was 18.0±11.0 cm (range, 6.0–56.5 cm), and according to the FNCLCC grading system for RPS, the patients were classified as follows: nine patients (18.8%) as grade I, 15 patients (31.2%) as grade II, and 10 patients (20.8%) as grade III. Liposarcoma (70.8%) was the most common histology, followed by leiomyosarcoma (16.7%). Thirty-five patients (72.9%) underwent R0 or R1 resection, and three patients (6.3%) underwent R2 resection. No patients received neoadjuvant radiation therapy or chemotherapy. However, 10 patients (20.8%) received radiation therapy and eight patients (16.7%) received chemotherapy after primary resection. Approximately 56.3% of patients underwent contiguous organ resection, and 29.2% had pathologic organ invasion. The 5-year OS rate after primary resection was 58.1% as shown in Fig. 2. The mean OS was 103 months (range, 0–203 months). The prognostic factors of OS after primary resection are shown in Table 2. Upon multivariate analysis, histologic grade (P=0.006) and chemotherapy after tumor resection (hazard ratio, 4.239; 95% confidence interval, 1.432–12.548; P=0.009) were significant prognostic factors for OS. The patients who received chemotherapy after resection were significantly associated with poor prognosis. The 5-year cumulative reoperation rate after primary resection was 62.5% as shown in Fig. 2.

Outcomes after primary resection of retroperitoneal sarcoma. (A) Overall survival rate. (B) Cumulative reoperation rate (n=48).
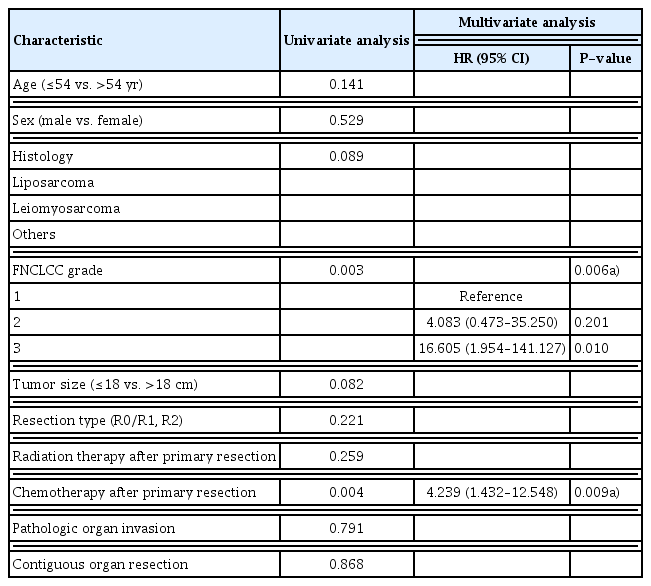
Prognostic factors for overall survival after primary resection for retroperitoneal sarcoma (n=48)
Prognostic factors after second resection
Among the 48 patients who underwent primary resection at our institution, 23 patients (47.9%) underwent secondary resection for recurrence. The clinicopathologic characteristics of these 23 patients are shown in Table 3. The mean age was 58 years (range, 28–75 years). As in the primary resection group, liposarcoma (78.3%) was the most common histology. According to the FNCLCC grading system, six patients (26.0%) were classified as grade I, four patients (17.4%) were classified as grade II, and eight patients (34.8%) were classified as grade III. Twenty-one patients (91.3%) underwent R0 or R1 resection, and two patients (8.7%) underwent R2 resection. Three patients (13.0%) received radiation therapy and five patients (21.7%) received chemotherapy after secondary resection. The 5-year OS rates after secondary resection for RPS was 64.3% as shown in Fig. 3. Compared with the primary resection group, histologic grade had less prognostic significance (P=0.074) (Table 4) after the second resection for recurrence in multivariate analysis.

Clinicopathologic characteristics of patients who underwent secondary resection for recurred retroperitoneal sarcoma
Overall survival rate after second resection of recurred retroperitoneal sarcoma (n=23).

Prognostic factors for overall survival after secondary resection for recurred retroperitoneal sarcoma (n=23)
Subgroup analysis on repeated resections for recurrent retroperitoneal sarcoma
Of the 48 patients, 23 patients (47.9%) underwent 2nd resection for recurrence, 16 patients (33.3%) underwent 3rd reoperations, and nine patients (18.7%) underwent additional resections for repeated recurrences (Fig. 4). The median surgery-free survival after repeated resections is shown in Fig. 5. As the number of repeated resections for recurrent RPS increased, the median surgery-free survival rate tended to decrease; however, there was no significant correlation between the number of repeated resections and surgery-free survival. The 5-year OS rate for patients operated on only once, twice, and more than three times were 51.4%, 57.1%, and 75.0%, respectively, indicating that number of repeated operations may not be associated with prognosis, even though our number of patients was small (Fig. 6).

A 51-year-old female patient at diagnosis who underwent repeated resections for dedifferentiated liposarcoma. (A) 3rd operation, (B) 4th operation, (C) 5th operation, and (D) 6th operation.

Median surgery-free survival in reoperations of recurred retroperitoneal sarcoma.

Overall survival rate of patients who underwent resection for retroperitoneal sarcoma.
In the case of liposarcoma, well-differentiated liposarcoma can dedifferentiate, which is associated with more aggressive clinical behavior [14]. Among 14 patients who underwent reoperations for recurrent liposarcoma, histologic type change from well-differentiated liposarcoma to dedifferentiated liposarcoma was reported in three patients (21.4%). Five patients (35.7%) were diagnosed with well-differentiated liposarcoma, and six patients (42.9%) were diagnosed with dedifferentiated liposarcoma without histologic type change. There was a tendency towards decreased survival when well-differentiated liposarcomas underwent dedifferentiation (Fig. 7).
Overall survival rate dependent on histologic type of liposarcoma (n=14). WD, well-differentiated; DD, dedifferentiated.
DISCUSSION
Previous studies have documented several factors which contribute to higher OS for RPS, and tumor grade was regarded as one of the most important independent predictive factors. Accordingly, our results also indicated that the FNCLCC tumor grade was the only independent prognostic factor for OS [2,11,13,15–21]. Tumor grade can also assist clinicians in determining the follow-up strategies, because the risk of recurrence is highly associated with tumor grade. In other studies [17,22,23], histologic type was also a significant factor for OS. Our results showed that in the primary resection group, liposarcoma had better prognosis compared to other histologic type tumors in univariate analysis, but there was no statistically significant difference in OS upon multivariate analysis. These results may be due to a relatively small number of cases with the majority being liposarcomas.
Currently, the role of systemic therapy or radiation therapy for RPS remains unclear [20,24–26]. There are studies reporting that postoperative radiation therapy may be related to improvement of local recurrence in RPS patients [15,27]; however, there is no clear evidence that radiation therapy improves OS. Also, neoadjuvant radiotherapy with or without chemotherapy may also have a beneficial role in selected cases [28]. In our patients, adjuvant chemotherapy or radiation therapy was selectively used in cases when complete resection was not possible or when the risk of recurrence was estimated to be high after resection. No significant difference was noted between the patients who were treated with adjuvant radiation therapy and those who were not. Miura et al. [29] studied 8,653 patients with surgically resected RPS and reported that currently available chemotherapy regimens for RPS do not provide survival benefits. In our study, the patients treated with chemotherapy after primary resection had a worse prognosis. This is most likely because the patients with severe disease progression received chemotherapy. In seven out of eight patients who received chemotherapy, the FNCLCC tumor grade was II or III, and the median OS of these patients was 11.5 months (range, 4–106 months).
It is generally recognized that another major prognostic factor related to survival outcome is whether complete resection of the tumor was performed [6,16,18,19,21]. In this study, R0 or R1 resection with a curative intent was mainly performed for most patients; however, three out of 16 patients (18.8%) who underwent resections more than three times had R2 resection more than once. The median OS rate after primary resection of these patients was 109 months (range, 92–138 months) until the follow-up period. There was no significant difference in OS according to the type of resection, suggesting that even with R2 resection, surgical treatment attempts to reduce tumor burden may be beneficial.
The unique feature of this paper is that we studied the median surgery-free survival in 23 patients who underwent repeated resections for recurrence. After primary resection, the median surgery-free survival was 25.5 months (range, 3–109 months), and as the number of reoperations increased, the median surgery-free survival tended to decrease, indicating earlier recurrence after repeated resections for recurrence. However, a statistically significant difference was not noted. An interesting point of our study is that patients who underwent repeated resection for recurrence had better OS compared to patients who underwent single resection for RPS. In fact, our results indicated that patients who underwent resections more than three times for recurrence tended to have better OS compared to patients who were operated on once or twice, although statistical significance was not reached because of the small number of patients. This finding suggests that even when RPS recur, when the recurrent tumor is amenable to surgical resection, OS may be improved, in contrast to unresectable recurrence. Our finding again emphasizes the central and most important role of surgical intervention in management of RPS. Aggressive repeated surgical approach until the point of unresectable recurrence is warranted.
In some cases of liposarcoma, histologic changes from well-differentiated type to dedifferentiated type occurred. The clinical behavior of dedifferentiated liposarcoma involves aggressive local growth and increased risk of local recurrence and tumor-related death [14]. In this study, among 14 patients who needed repeated resections for liposarcoma, there was a histologic type change from well-differentiated to dedifferentiated liposarcoma in three patients (21.4%) with a 5-year survival rate of 66.7%. There was a significant difference for 5-year survival between well-differentiated liposarcoma and dedifferentiated liposarcoma with no histologic type change (P=0.031). A previous study involving 135 patients with retroperitoneal liposarcoma reported that dedifferentiation was the most significant risk factor which influenced survival [30]. The mechanism of transformation from well-differentiated liposarcoma to dedifferentiated liposarcoma is not clear [20]. However, in case of histologic type change to dedifferentiated liposarcoma, this may affect the survival of patients with liposarcoma.
This study had some potential limitations. First, the retrospective design might have led to selection bias. Second, the number of patients included in this study was relatively small. Third, the proportion of patients who received radiation therapy or chemotherapy was small, limiting the evaluation of effectiveness of adjuvant therapy.
In conclusion, according to the results of this study, the 5-year OS rate after primary resection at our institution was 58.1%, and 5-year cumulative reoperation rate after primary resection at our institution was 62.5%. Only the FNCLCC grade was a significant prognostic factor for OS. The 5-year OS rate for patients who underwent more than 3 repeated resections was 75.0%, which is comparable to patients who underwent resection only once or twice. In addition, radiation therapy or chemotherapy after resection had no effect on survival. Although OS for patients with RPS remains poor, our study shows that repeated resection in comparison to single resection does not decrease the 5-year OS rate of patients with recurrent RPS. Therefore, aggressive surgical strategies for recurrent RPS patients are warranted.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.