INTRODUCTION
Low-grade endometrial stromal sarcoma (ESS) is typically a uterine mesenchymal neoplasm but it may also occur in extrauterine sites. Extrauterine ESS (EESS) is rare and the exact incidence is unknown. The majority of these cases are associated with endometriosis and have a relatively higher tendency to disseminate than uterine ESS. The commonest extrauterine site of origin is the gastrointestinal tract, but cases from the pelvis, sciatic nerve, vulva and retroperitoneum have also been reported [1]. ESS arising in the vagina is a rare entity. The diagnosis may be difficult owing to associated endometriosis that presents with similar clinical features. We report a case of low-grade EESS arising in vaginal endometriosis. This case merits mention because of the difficulty in diagnosis due to overlapping clinical features and response to medical therapy, timely management, and good survival outcomes. An informed written consent was obtained from the patient for the publication of this report.
CASE REPORT
A 38-year-old P2L2 patient presented with complaints of dyspareunia, dysmenorrhea, and painful defecation for a year, along with blood-mixed vaginal discharge for 3 months. Her systemic examination was normal. On per speculum examination, the cervix was normal but multiple brownish irregular nodules were seen in posterior vaginal fornix. On bimanual examination, fixed tender nodules were felt in the posterior fornix with irregularity in the overlying vaginal mucosa. The uterus was retroverted, normal-sized with restricted mobility. Examination during menstruation noted the presence of blood-mixed mucoid discharge from the nodules in the posterior fornix (Fig. 1A). With clinical suspicion of vaginal endometriosis, imaging and biopsy were performed. Computed tomography pelvis showed normal uterus and adnexa with nodularity and thickening of posterior vaginal fornix with ill-defined planes posteriorly with rectum (Fig. 1B). Biopsy of the irregular nodular areas in posterior fornix showed proliferative endometrial glands and cellular stroma suggestive of extrauterine endometriosis (Fig. 1C).
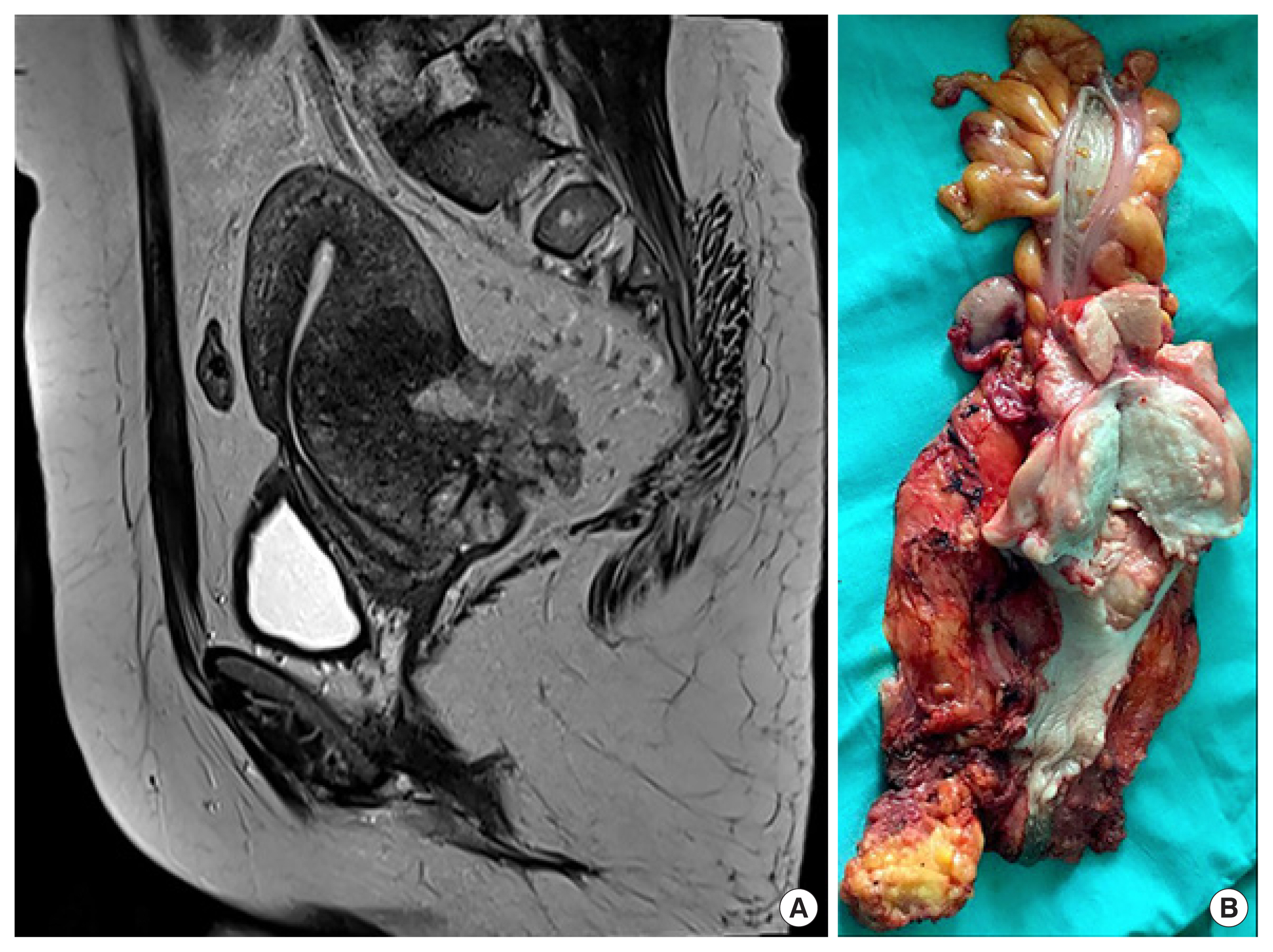
The patient opted for medical therapy and was started on leuprolide acetate 3.75 mg intramuscular injection monthly for 3 months. There was a significant improvement in her symptoms with disappearance of the vaginal forniceal lesions. Thereafter, the patient was started on depot intramuscular injection of medroxyprogesterone acetate 150 mg every 3 monthly for 12 months. Eighteen months after diagnosis, she presented again with blood-mixed vaginal discharge for 3 months with dyspareunia and dyschezia. On per speculum examination, there was an irregular exophytic necrotic growth in posterior vaginal fornix. The cervix appeared normal. On bimanual examination, a hard fixed mass was felt posteriorly in the rectovaginal septum. The uterus was normal in size with restricted mobility. On rectal examination, the mucosa was free with external compression by the mass. A repeat biopsy from necrotic growth in the posterior fornix was suggestive of low-grade ESS. Magnetic resonance imaging showed a T1 isointense and T2 heterogeneously enhancing hyperintense mass of 7×6 cm in the rectovaginal septum with an exophytic component and necrosis with diffusion restriction (Fig. 2A).
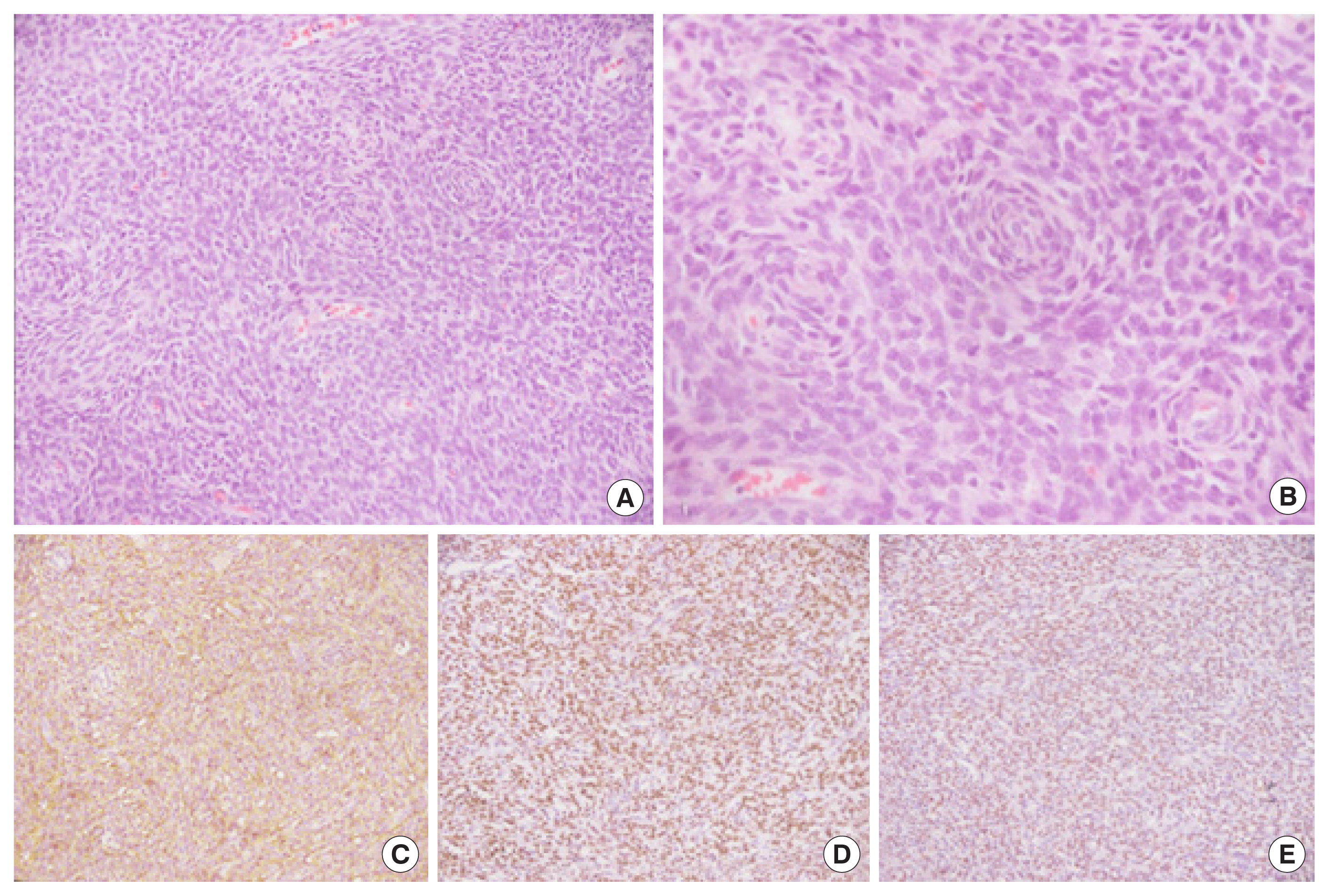
The patient was taken up for laparotomy. Intraoperatively, the pouch of Douglas was obliterated by a fixed mass of 7×5 cm arising from the posterior vaginal wall and rectovaginal septum filling the pouch of Douglas, encasing the left ureter and invading the rectosigmoid. Inferiorly, the tumor was extending almost up to 4–5 cm from the anal sphincter. A retrograde hysterectomy with excision of posterior vaginal wall, abdominoperineal resection of rectosigmoid colon and a permanent end colostomy was performed (Fig. 2B). Gross histopathological examination of the specimen showed a 7.5×5.5×3 cm grey-white tumor involving the rectovaginal septum, infiltrating the serosal aspect of rectosigmoid, posterior myometrium up to endometrium isthmus and part of cervix. The cut end of vaginal cuff, colonic and rectal margins were free of tumor. Bilateral tubes and ovary were normal with no evidence of endometriosis. The tumor cells were immunopositive for CD10, ER, PR and focally for cyclin D1 and desmin, while negative for SMA, consistent with a diagnosis of ESS (Fig. 3). There were foci of endometriosis found embedded within the periphery of the tumor. The patient recovered uneventfully and was discharged on third postoperative day. The patient was diagnosed with stage IIIA low grade, EESS of the vagina and was started on the aromatase inhibitor anastrozole 1 mg daily. The patient was followed up in a combined oncology clinic every month for the first 3 months; 3 monthly till 2nd year and 6 monthly till the 5th year. At every visit, a careful evaluation of symptoms was done, thorough clinical examination was performed and imaging was advised accordingly. She also underwent dual-energy X-ray absorptiometry scan every 1–2 yearly to monitor bone mineral density. She was on calcium and vitamin D supplementation and was provided advice on a healthy lifestyle and importance of regular physical exercise. At 65 months follow-up, the patient is disease-free. We plan to continue anastrozole therapy till disease progression or development of significant toxicity in terms of osteopenia/osteoporosis.
DISCUSSION
Malignant transformation of long-standing endometriosis occurs in 0.7% to 1% of cases and the most common histopathology is adenocarcinoma, particularly of the endometrioid or clear cell subtype. Rarely endometriotic foci can give rise to ESS. EESS arising from endometriosis is an extremely rare condition, reported only in few case reports. The symptoms of ESS and endometriosis are similar and depend on the site of involvement.
EESS can arise as a primary disease as a result of metaplasia of sub-coelomic mesenchyme or secondarily from malignant transformation of pre-existent endometriosis. It may not always be possible to differentiate primary EESS from secondary EESS. According to Sampson criteria, to diagnose endometriosis-associated malignancy, the following points should be met: (1) demonstration of benign endometriotic foci in the proximity of the malignant tumor; (2) no other primary site for the tumor; or (3) histology of tumor consistent with origin from an endometriotic foci [2]. Our case met all of Sampson’s criteria (presence of multiple endometriotic foci in the periphery of the tumor, presence of tumor in rectovaginal septum and posterior vaginal wall excluding any other source of primary origin, histopathological examination consistent with that of ESS arising from endometriosis) suggesting that the initial vaginal endometriosis had undergone malignant transformation into low-grade ESS subsequently. It has also been noted that it is not always necessary to identify a focus of endometriosis near the tumor because growth of tumor may destroy the transitional areas of endometriosis. Therefore, any tumor of histological type known to be associated with endometriosis occurring at an unusual age and at an uncommon site may point towards the diagnosis of malignant transformation even without a demonstrable focus of endometriosis in real time.
One of the most important differential diagnoses to be considered is gastrointestinal stromal tumor (GIST). GISTs are rounded smooth tumors, arising as an endoluminal, exophytic growth. They are immune positive for CD117 and DOG-1. In comparison, the characteristic appearance of gastrointestinal tract ESS is that of an extrinsic mass that may involve the complete thickness of rectal wall with luminal protrusion. The presence of invasive tongues of tumor at the periphery of the neoplasm, short fascicles or sheets of monotonous plump spindle cells and prominent arterioles favor the diagnosis of ESS.
Most common site of origin of EESS are the ovaries. Only few cases were reported arising from the vagina (Table 1) [1,3–15]. ESSs are characterized by the presence of the fusion of JAZF1 and SUZ12 (JJAZ1) genes resulting from translocation of t(7,17)(p15;q21). But, in contrast, EESS rarely harbors this genetic abnormality.
The factors that lead to malignant transformation in endometriosis are not clear. Exogenous hormone therapy with estrogen was considered as a potential contributing factor for the development of the colonic ESS in a few case reports. Conversely, hormonal therapy may have checked the tumor growth as medroxyprogesterone acetate is known to achieve tumor control in already diagnosed cases of ESS. Our patient was given hormonal treatment with gonadotropin-releasing hormone (GnRH) analogs and progesterone as she was initially diagnosed to have deeply infiltrating rectovaginal endometriosis. Low-grade ESS is a slow growing neoplasm and the management is primarily surgical with the aim of complete cytoreduction. The most important prognostic variable is stage with 5-year survival rates as good as 90% to 100% for stage 1 and reduced to 50% for advanced stage disease. A systematic review on EESS has revealed that small size of the tumor and hormonal therapy were predictors of a good survival, while the role of chemotherapy or radiation does not seem to affect survival. In cases of disseminated intraperitoneal disease survival rates as low as 12% have been reported. Late recurrences are common, even with early-stage tumors, mandating a long time follow-up for these patients.
In conclusion, being an extrauterine foci of endometriosis, any primary tumor of the endometrium might arise from endometriosis. A practicing gynecologist should keep this rare possibility in mind while medically treating long-standing cases of deeply infiltrating endometriosis. Features suggestive of malignant transformation include worsening symptoms, development of resistance to a previously responsive medical treatment or sudden increase in size.