INTRODUCTION
As long-term oncological safety has been confirmed over time, laparoscopic or robotic gastrectomy has become a standard option in treatment of early gastric cancer (EGC) [1,2]. EGC is defined as a malignancy invading the mucosa and submucosal layer, regardless of lymph node metastasis [3]. Because of the shallow depth of the tumor, it is difficult to determine the exact location of the lesion by simply touching the serosa with surgical instruments during total laparoscopic or robot surgery [4]. Therefore, it is important to use an adequate tumor localization method to ensure adequate proximal resection lines during intracorporeal anastomosis.
For total laparoscopic or robotic surgery, there are several methods for localization of the tumor [5–7], such as endoscopic tattooing, intraoperative endoscopy, or ultrasonography. However, the blurring effect of tattoo ink or need for additional equipment and endoscopists for intraoperative endoscopy have made the preoperative endoscopic clipping method the most popular option [4].
The location of the clips can be identified with abdominal radiographs (abdominal X-ray, AXR) before surgery and can be confirmed with intraoperative AXR when the surgeons cannot determine an adequate resection line during the operation. Intraoperative AXR can be performed easily and safely. However, it can be time consuming during surgery, and there are concerns of additional radiation exposure [8].
These disadvantages lead us to question the usage of additional AXR during the operation. Through this study, we compared the outcomes between patients who did not undergo intraoperative AXR before gastric resection and those who did.
METHODS
Patients and preoperative localization procedure
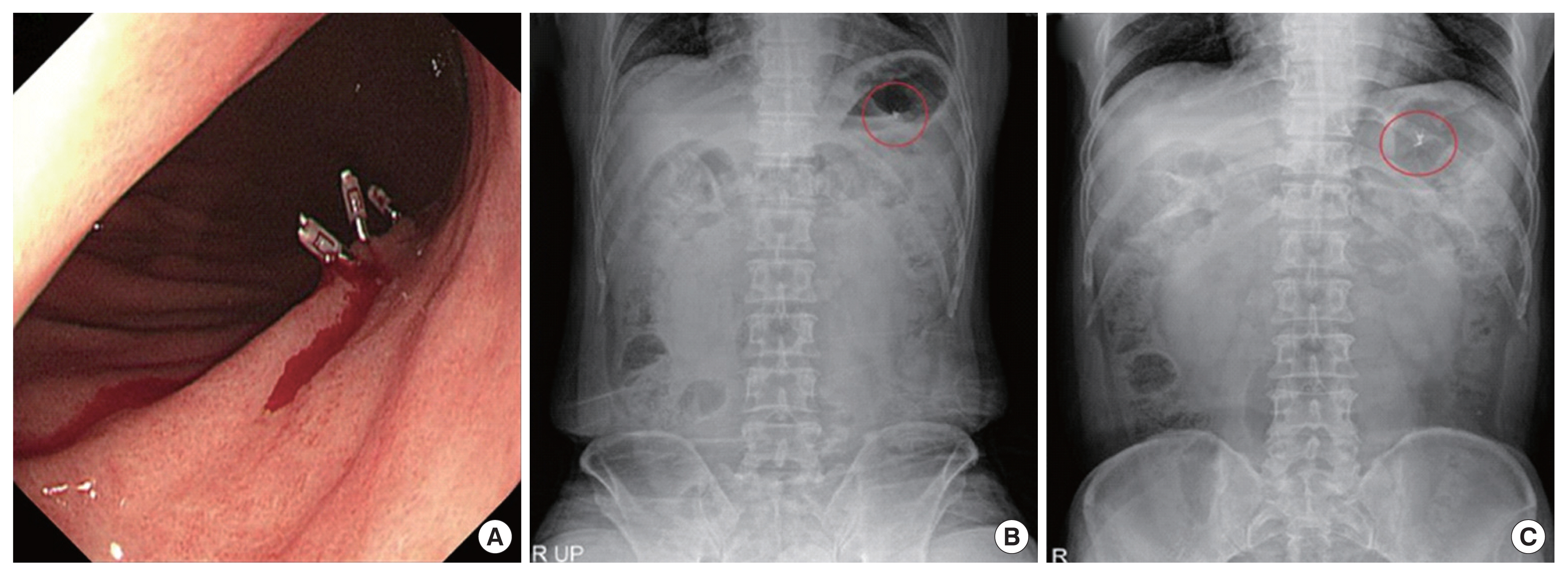
Patients (n=926) with clinical EGC who underwent laparoscopic or robotic gastrectomy and intracorporeal anastomosis at Samsung Medical Center from September 2012 to September 2018 were enrolled in this study. Among them, 331 patients with tumor above the stomach angle underwent preoperative clipping localization with esophagogastroduodenoscopy (EGD), and more than 2 metal clips were applied approximately 1 cm above the lesion before or in the early morning of the day of the operation. Immediately after clipping, AXR including supine and erect positions was performed to confirm the location of the clips (Fig. 1).
Intraoperative localization procedure
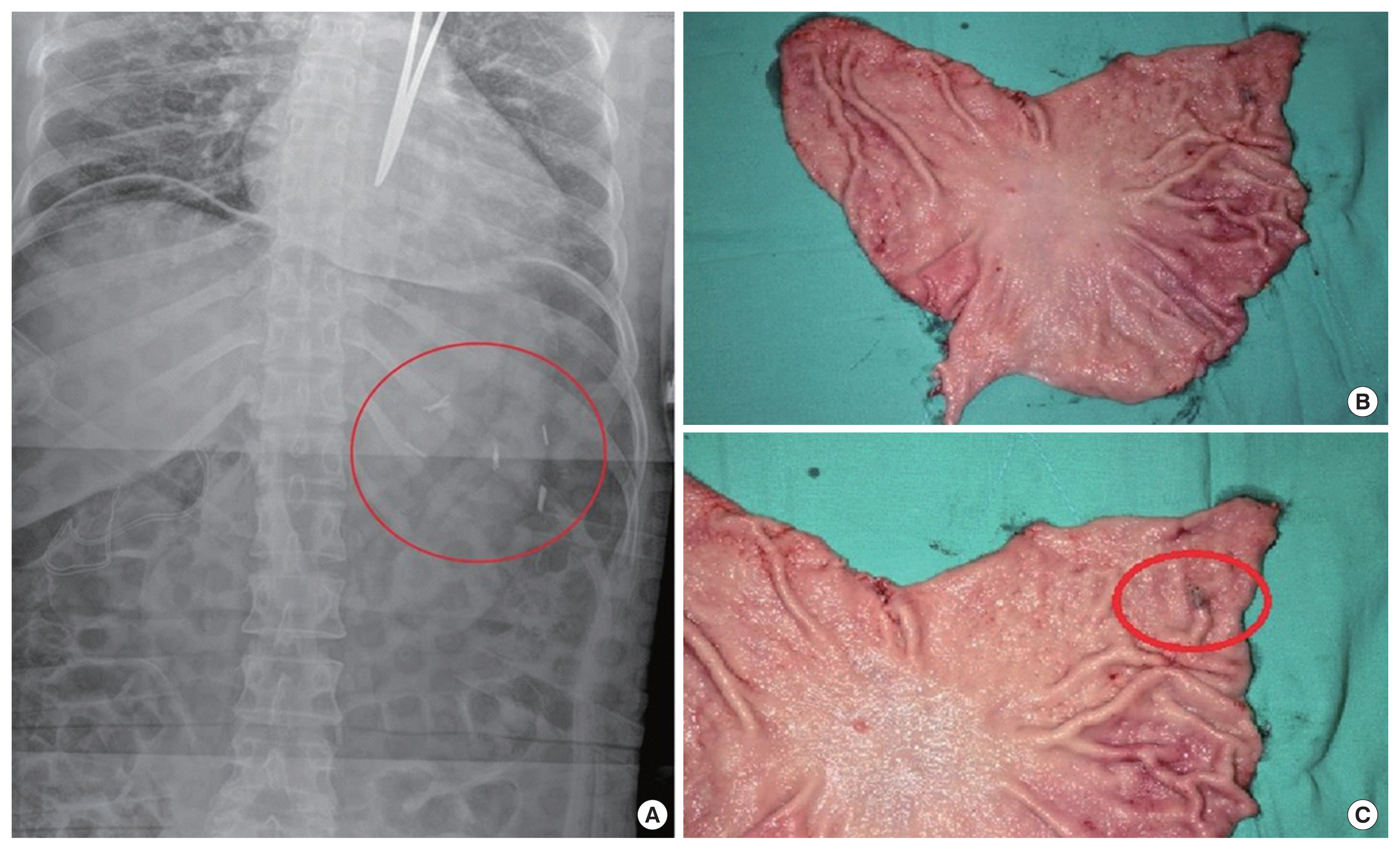
During the operations of 251 patients (group A), the location of the clips was estimated based on multiple images of preoperative EGD and AXR. Intraoperative AXR was not performed before gastric resection for those patients. Landmarks were angled when the tumors were located on the lesser curvature side and gastric rugae when the tumors were located on the greater curvature side. The distances between those landmarks and the tumors were estimated with the length of the endoscopic tube from the esophagogastric junction to the tumors. After gauging the location of the tumors based on preoperative EGD and AXR, laparoscopic metal clips were additionally applied in 80 patients (group B). The metal clips were applied at the greater curvature and lesser curvature of the stomach surface. After intraoperative AXR, a surgeon confirmed whether the endoscopic clips were located between the laparoscopic metal clips (Fig. 2). A line was drawn on the stomach wall to visualize the proximal resection margin (PRM), which was located between the metal clips and at least 2 cm from the endoscopic clips.
Confirmation of the clips on the specimens
After resection of the stomach, the specimen was retrieved from the abdominal cavity. After identification of the clips and the tumor, frozen biopsy was performed on the proximal margins to confirm the presence of cancer cells. The PRM (cm) was defined as the shortest length between the tumor and the proximal resection line. If the resection margin was positive for malignancy, additional resection was performed.
We retrospectively analyzed the clinicopathologic characteristics (age, sex, use of intraoperative AXR, tumor location, tumor size, histologic type, type of gastrectomy, and reconstruction) and outcomes (result of frozen biopsy, re-resection, and PRM) of the preoperative clipped patients on the basis of medical records and pathologic reviews.
The study was approved by the Institutional Review Board of Samsung Medical Center (IRB No. SMC 2019-01-095).
Statistical analysis
Differences in clinicopathologic parameters and outcomes between patients in groups A and B were determined by t-test, chi-square test, and Fisher exact test. After evaluating the receiver operating characteristics and area under the curve (ROC and AUC) of the variables significantly associated with outcome, we used Youden indices to determine the optimal cutoff value of the continuous variables. The factors significant in univariate analysis were confirmed with multivariate logistic regression analysis. P<0.05 was considered statistically significant. Statistical analysis was carried out using the statistical software SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
The clinicopathologic characteristics, operation data, and outcomes of the preoperative clipped patients (n=331) are described in Table 1. Tumor location had no significant difference in both groups A and B, and was distributed mostly at the middle portion of the stomach (83.3% vs. 92.5%, P=0.052). Tumor size was also significantly larger in group B compared to group A (3.2 cm vs. 2.6 cm, P=0.046). Sixty-five percent of the patients in group B underwent Billroth I anastomosis after gastrectomy, and 75.7% of the patients in group A underwent Billroth II anastomosis (P<0.001). The rate of positive frozen biopsy in group B was 3.8% (n=3), while that in group A was 2.8% (n=7). The rate of additional resection was significantly higher in group B (7/80, 8.8%) compared to group A (7/251, 2.8%) (P=0.048). The mean length of the PRM was 2.4 cm in group B and 3.3 cm in group A, a statistically significant difference (P<0.001).
The factors associated with positive frozen biopsy results and additional resection rate are shown in Table 2. Ten cases (3.0%) were confirmed with tumor positive frozen biopsy results, and 14 patients (4.2%) underwent a re-resection procedure during operation. After extraction of the specimen from the abdominal cavity, four patients (1.2%) had to undergo re-resection due to short PRM (<0.5 cm), regardless of negative frozen biopsy results.
Two out of four patients underwent additional 2 cm resection, and frozen biopsy was performed on the PRM to confirm a negative result. The other two patients underwent total gastrectomy because the location of the lesion was proximal midbody, which was close to the cardia.
The mean tumor size was 2.7 cm in patients with negative frozen biopsy results, and 5.5 cm in patients with positive frozen biopsy results (P=0.035). Although it was not statistically significant, the proportion of undifferentiated histologic type was higher in patients with positive frozen biopsy results. Tumor size of patients who had to undergo re-resection was significantly larger than that of those who did not have the re-resection procedure (4.9 cm vs. 2.6 cm, P=0.032).
The ROC and AUC of tumor size in predicting the possibility of re-resection were 0.715 (95% confidence interval [CI], 0.58–0.84; P=0.007). The cutoff value of the tumor size was 2.4 cm with a Youden index of 0.362. The multivariate analysis in Table 3 shows that tumor size was significantly associated with positive frozen biopsy results (odds ratio [OR], 1.48; 95% CI, 1.18–1.85; P<0.001), and tumor larger than 2.4 cm was significantly associated with re-resection (OR, 5.53; 95% CI, 1.17–26.30; P=0.031).
DISCUSSION
We compared the results of frozen biopsy, additional resection rate, and PRM to investigate whether intraoperative AXR was useful in determining adequate resection lines. This study showed no significant difference in outcome between patients who underwent intraoperative AXR and those who did not. This finding suggests that intraoperative AXR is not necessary to obtain safe resection margins during laparoscopic or robotic gastrectomy and intracorporeal anastomosis.
In total laparoscopic or robotic surgery with endoscopic clipping, it is difficult to confirm the location of the clip by touching the serosal surface in the operation field. To complement this, endoscopic dye injection, intraoperative endoscopy, laparoscopic ultrasonography, and intraoperative radiography have been proposed.
Indigo carmine dye injection through endoscopy can cause a spreading out of the lesion over time after injection and can lead to blurring of the border. The indocyanine green (ICG) method requires additional expensive equipment for ICG detection and cannot be used in patients with contrast allergies [9]. In addition, uncommon complications may occur after endoscopic staining, such as abscess forming peritonitis, fat necrosis, inflammatory gastritis, and chemical peritonitis [7,10,11]. Laparoscopic ultrasonography and intraoperative endoscopy require specific endoscopic skills and devices. In addition, because of the inability to obtain a visual field during surgery due to bowel distension, additional procedures are needed to decompress the gas in the intestine or to clamp the proximal jejunum so that air does not descend into the jejunum [6].
Despite the disadvantage of additional endoscopy once before surgery, preoperative endoscopic clipping is often used to localize the non-palpable EGC lesion, to obtain an adequate resection line, and minimize the unnecessary length of the PRM [4]. To determine the location of the preoperative applied clip during the operation, we frequently use intraoperative AXR. This method does not require specific skills or devices compared to other methods and is a cost-saving method [8]. However, there are concerns of unnecessary radiation exposure to the patient and the medical team. In addition, by omitting this process, we can reduce the operating time for the radiographer. As a result, we investigated the necessity of intraoperative AXR.
In addition to identifying clips during the operation and avoiding tumor positive frozen biopsy results and re-resection procedures, it is important for endoscopists to clip the anatomical “proximal” margin and not the “lateral or around” margin of the tumor. To easily identify the location of the clips, the standard view of EGD is important. These standard EGD views should include the esophagogastric junction, angle, or gastric rugae. Although it was not statistically significant, undifferentiated gastric cancer was more frequent in patients with positive frozen biopsy. Undifferentiated tumors may have poor demarcated margins, and this factor can make it difficult for endoscopists to identify the appropriate place to clip. Furthermore, in previous studies, large tumors were significantly associated with positive resection margin, and large size was a risk factor for this result [12,13]. We also found that large tumor was significantly associated with re-resection. Based on these results, we suggest that endoscopic clipping should be performed 1 cm or more proximal to the tumor.
Since we did not have detailed protocol for endoscopic clipping in our center, important standard views of EGD with clips could not be retrieved, which may affect the results after gastrectomy. In addition, it is unfortunate that we did not have the data of accurate measurements between the predicted location of the endoscopic clip and anatomical landmarks of the stomach during laparoscopic or robotic surgery.
We analyzed a small number of cases performed by only two surgeons (JHL and JYA) in this study. Therefore, there might be selection and information bias with a limitation in generalization of this result to other hospitals or surgeons.
In addition, there are differences in anastomosis methods between groups and the position of tumor is higher in group B, which may act as a bias in the analysis. In group A, 212 of 251 patients (84.5%) were JHL’s patients, and in group B, all 80 patients (100%) were JYA’s. According to the operator’s preference for anastomosis method, group A had a high Billroth II anastomosis rate (75.7%) and group B had a high Billroth I anastomosis rate (65%). In comparison with Billroth I, Billroth II anastomosis would often not require intraoperative AXR, because it is possible to obtain enough PRM even if gastrectomy is performed without intraoperative AXR. And in tumor location, although there was no statistically significant difference between the two groups, group B (93.8%) had a higher tumor location than group A (84.1%). If the location of the tumor was not high enough to clearly determine the resection line with the preoperative AXR alone, no additional intraoperative AXR would be necessary.
In conclusion, intraoperative AXR is an unnecessary method for obtaining safe PRM with negative frozen biopsy results, only when it is possible to predetermine the resection line with preoperative AXR. Also, we suggest that the endoscopic clip should be placed 1 cm or more proximally, especially in large, poorly differentiated cancers. The location of the clips should be estimated by correlation with preoperative AXR and standard views of the EGD.